

Before your next transfer, your clinic may have suggested an endometrial scratch.
It is a small procedure, performed in the cycle before transfer. A thin catheter is passed through the cervix and a small area of the uterine lining is abraded — scratched — creating a localised injury. It takes a few minutes and can cause cramping similar to period pain, which usually resolves within hours. The scratch can also be performed during a diagnostic hysteroscopy, where the same instrument used to inspect the uterine cavity creates the injury at the point of withdrawal.
The procedure has a more layered biological rationale than it first appears.
Why the scratch is offered
The theory behind the endometrial scratch operates on several levels.
The first is the repair response. When tissue is injured, the body sends resources to fix it — increased blood flow, growth factors, immune activity. The theory is that this repair activity leaves the lining in a more receptive state when the embryo arrives the following cycle.
The second is that the scratch may trigger a process that prepares the lining to receive and hold an embryo — helping it form the right environment for attachment, controlling how deeply the embryo embeds, and supporting the immune tolerance that allows the embryo to stay rather than be rejected.
The third is timing. IVF stimulation can push the lining ahead of where the embryo is — the two are slightly out of sync at the point of transfer. The scratch in the previous cycle may help reset that timing.
These are plausible biological reasons for the procedure. The question the regulator addresses is whether they translate into more live births.
What the regulator assessment shows
The HFEA reviews each add-on against the evidence for whether it improves the chance of a live birth.
On the endometrial scratch, the published assessment is that the evidence does not currently support its use as a routine add-on for the general IVF population. Earlier studies suggested benefit, particularly in women with recurrent implantation failure, and the procedure became widely used on that basis. Larger, better-designed trials have not confirmed that benefit across the broader population. For women with recurrent implantation failure specifically, the picture remains less settled — some studies show signal, others do not.
The distinction matters. The HFEA assessment covers the general IVF population. If you have had multiple failed transfers, your situation sits in the subgroup where the evidence is more actively debated — and where a consultant’s specific rationale for the procedure carries more weight than a general recommendation.
The clinical situations where the scratch may still be considered are specific:
- Recurrent implantation failure where standard preparation has not produced a successful transfer and a consultant has a specific rationale for the procedure
- Individual cycle histories where the endometrial response has been atypical
- Where a diagnostic hysteroscopy is already planned and the scratch can be incorporated without additional intervention
If your recommendation came with that specific clinical picture behind it, the conversation with your consultant is a different one. If it was offered as a routine next step, the assessment is useful information to bring into that conversation.
The regulator’s work is designed to inform that conversation, not replace it.
What the repair response needs
The scratch creates the stimulus. Nutrients activate the response.
Each of the mechanisms the scratch is intended to trigger — repair, immune modulation, the preparation of the lining for attachment — draws on what the body has available. Zinc is a documented cofactor in cell proliferation and the formation of new tissue. A body well-supplied with the nutrients these processes depend on responds differently to the same stimulus than a depleted one. This is a gap that you can fill.
These are the same inputs implantation depends on when transfer comes.
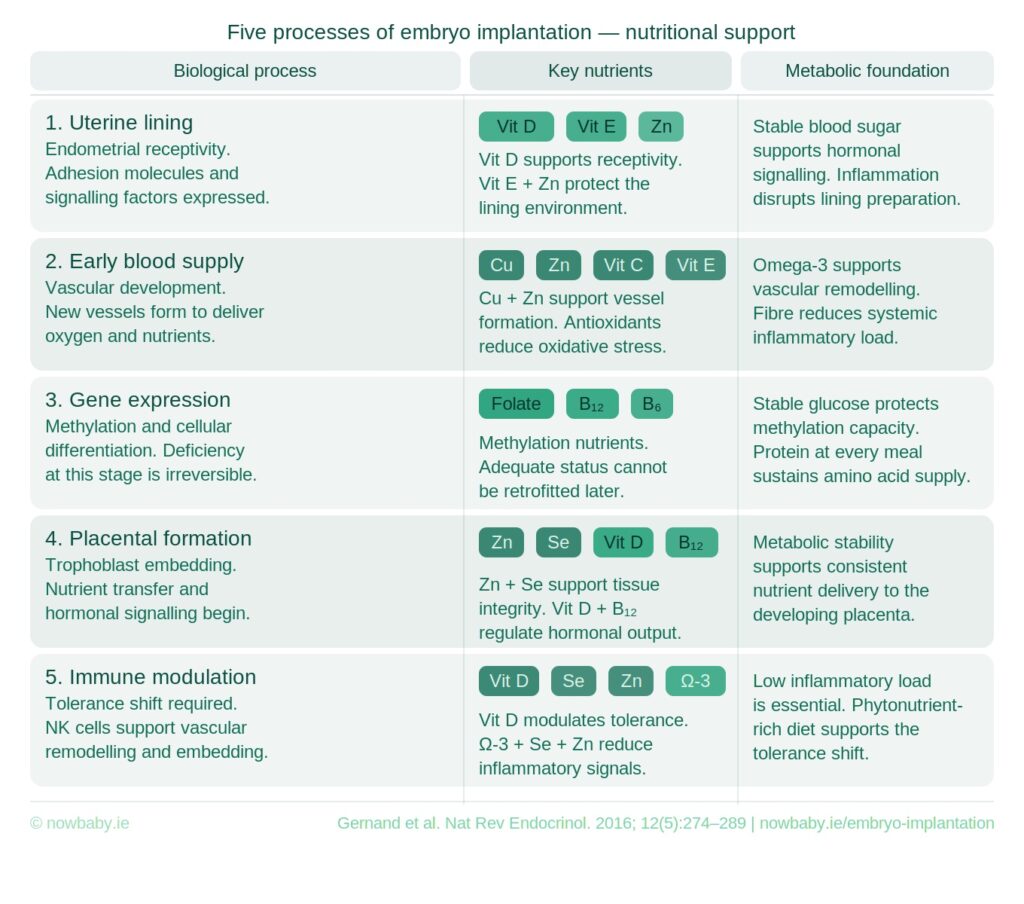
Around 2 in 3 frozen transfers do not result in a live birth. The two-week wait is not neutral — it is biologically active. Receptivity, early blood supply, placental formation, immune modulation — each stage has its own specific nutrient requirements.
 The Now Baby FET Implantation Meal Plan was built for targeted implantation support. Professionally analysed. Beginning the day after transfer.
The Now Baby FET Implantation Meal Plan was built for targeted implantation support. Professionally analysed. Beginning the day after transfer.
You didn’t come this far to wing it.






