

The Human Fertilisation and Embryology Authority, the UK’s independent fertility regulator, is one of the few public bodies anywhere in the world that publishes plain-English evidence reviews on the optional tests, treatments and laboratory techniques offered alongside standard IVF. They look at the trials, weigh the data, and tell patients and clinicians what the research currently shows. Their assessments are widely referenced internationally, regardless of where treatment is taking place.
PGT-A testing — preimplantation genetic testing for aneuploidy — is one of those add-ons, and one of the most widely offered.
What PGT-A is
PGT-A testing is performed on embryos before transfer. A small number of cells is taken from each blastocyst and analysed for the expected number of chromosomes. Embryos with the typical count are described as euploid. Those with an extra or missing chromosome are described as aneuploid.
The aim is to give clinicians better information when deciding which embryo to transfer first.
Where PGT-A has a clear clinical role
The strongest evidence for PGT-A testing sits in specific clinical situations.
Women in their late thirties or forties, where chromosomal errors in eggs become more common with age. Couples who have had multiple miscarriages where chromosomal causes have already been identified. Repeated cycles where good-looking embryos have failed to implant. Severe male factor infertility, where sperm-related chromosomal errors are more likely.
The reason age and egg-related factors dominate that list is biological. More than 90% of embryo aneuploidies originate from errors during egg development, not sperm. The egg sits in arrested meiosis for decades before ovulation, and that long pause is what makes it uniquely vulnerable. This is why PGT-A’s clinical case strengthens with maternal age, and why egg quality in the months before stimulation matters in any cycle, with or without testing.
In these situations, PGT-A is doing what it was designed to do. It identifies which of the available embryos carry the expected number of chromosomes, so transfer decisions can be made on better information. The relief of hearing this one is normal after a miscarriage, after multiple failed cycles, is real. The clarity matters.
What the regulator assessment shows
The HFEA reviews each add-on against the evidence for whether it improves the chance of a live birth.
On PGT-A testing, their published assessment is that the evidence does not currently support its use as a routine test for the average IVF patient. For some groups, the data suggest it may even reduce the chance of a live birth, because chromosomally normal embryos can still be discarded based on a biopsy that is not always representative of the whole.
This is not a verdict against the test. It is a statement about who the evidence supports, and who it does not.
If your clinical situation matches one of those above, the case for PGT-A testing in your cycle may be stronger than the general-population review suggests. If it does not, the assessment is useful information to bring into the conversation with your clinic about whether testing is the right next step.
The point of the regulator’s work is not to override clinical judgment. It is to give patients and clinicians a shared evidence base to discuss.
What no add-on can change
Whatever you and your clinic decide about PGT-A testing, one thing remains constant.
PGT-A does not improve the embryo you transfer. It selects from what is already there.
By the time the test can be performed, your cycle is largely already written. Stimulation has happened. Eggs have been collected. Some have fertilised and developed; some have not. Whatever number of blastocysts is left at biopsy is the group PGT-A acts on.
The number of eggs collected, how well they matured, the integrity of the sperm at fertilisation, the rate of attrition through the lab — those are shaped in the months before the cycle, by biology that responds to nutrition, hormonal signalling, sleep, stress and metabolic health.
Once a euploid embryo is selected and transferred, what happens next has nothing to do with the test either. Implantation depends on a body that is ready to receive the embryo. Pregnancy depends on the embryo’s own continuing development inside that body.
Even with a chromosomally normal embryo, more than 1 in 3 frozen transfers do not result in a live birth. The endometrial environment during the two-week wait is the variable that remains within your influence.
Evidence-based peace of mind for the two-week wait
The 2 Week Wait is not neutral, it is biologically active.
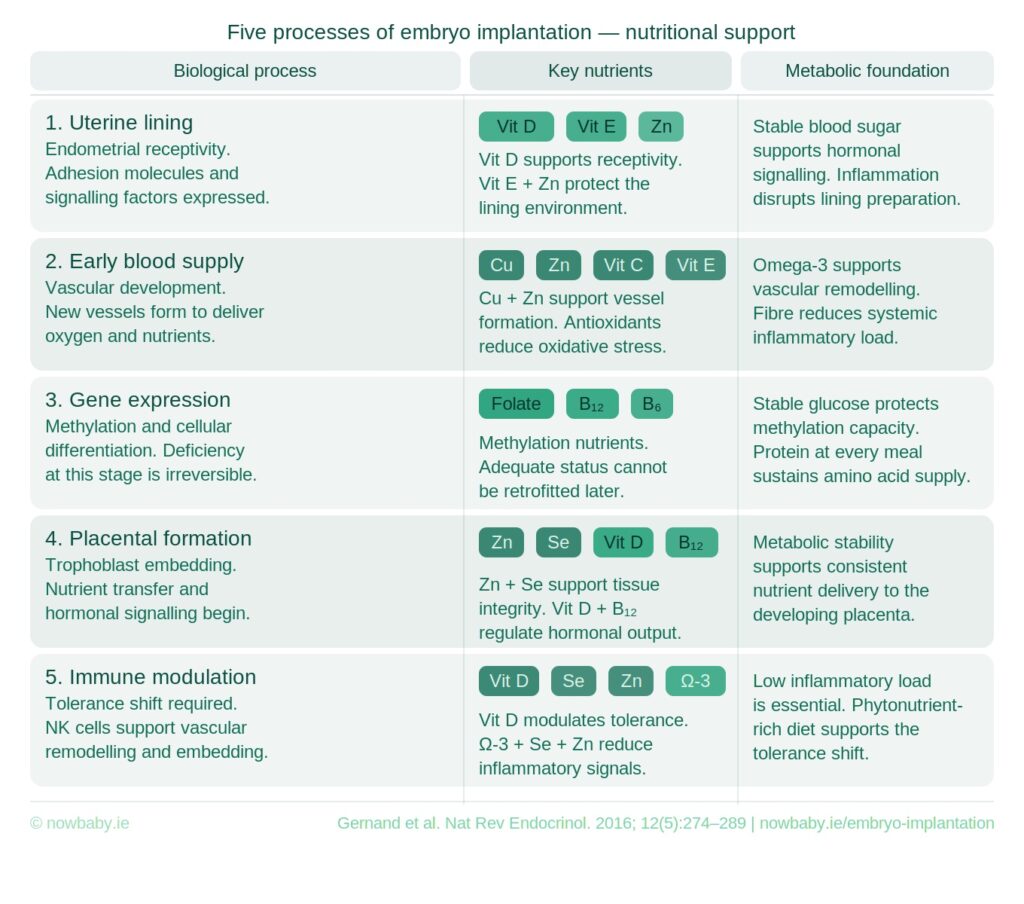
The Now Baby FET Implantation Meal Plan is structured to support each stage of implantation — secure embedding, early circulatory development, balanced immune signalling, and the early hormonal and metabolic conditions that pregnancy depends on. Every meal has been professionally analysed using clinical nutrition software so the macronutrient and micronutrient profile is balanced and consistent.
What it gives you is a decision already made. You are not standing in the kitchen during the most important fortnight of your cycle wondering whether what you are eating is helping. The plan has been designed for these specific days, by a fertility nutritionist, against the physiology of implantation. Your job is to follow it.
That is what evidence-based peace of mind looks like during the two-week wait. A clear nutritional structure to follow, designed for the biology you are in.

You didn’t come this far to wing it.





