The embryos were good. The transfers were done correctly. And each time, your embryo didn’t make it.
If you have been through this more than once, you already know that recurrent implantation failure is one of the hardest places to be in fertility treatment — because it explains almost nothing about why. Something is preventing implantation. The question of what is rarely answered clearly.
When it isn’t, the immune system is frequently proposed as the reason. And steroids — prednisolone or dexamethasone, prescribed to modulate immune activity around the time of transfer — are among the most commonly offered next steps.
The Human Fertilisation and Embryology Authority, the UK’s independent fertility regulator, is one of the few public bodies anywhere in the world that formally assesses the add-ons offered alongside standard IVF. Their evidence reviews are used internationally by clinicians and patients trying to understand what the research actually shows.
Steroids for recurrent implantation failure are on that list.
What the immune theory is based on
Implantation requires the maternal immune system to do something counterintuitive. It must partially suppress itself — tolerating an embryo that carries paternal antigens it would ordinarily identify as foreign.
The theory behind immune add-ons is that this balance is harder to achieve in some women. The immune environment remains more active than implantation requires. Steroids, as anti-inflammatory and immune-modulating agents, are offered to support that shift.
The reasoning has a biological basis. The question the HFEA addresses is whether intervening in that signalling produces more live births.
What the regulator assessment shows
The HFEA reviews each add-on against the evidence for whether it improves the chance of a live birth.
The evidence for steroids in recurrent implantation failure is weak. Routine use across the general population of women with implantation failure is not currently supported.
The clinical situations where the case for steroids may be stronger are specific:
- A diagnosed autoimmune condition — rheumatoid arthritis, lupus, thyroid autoimmunity — where immune dysregulation is already documented
- Endometriosis, where chronic peritoneal inflammation is part of the clinical picture
- Elevated inflammatory markers identified in blood tests that a consultant is specifically responding to
- A reproductive immunologist has reviewed the full picture and identified a specific immune pattern worth addressing
If your recommendation for steroids came with that level of clinical rationale behind it — a named condition, a specific test result, a specialist assessment — the conversation is a different one. The regulator’s assessment covers the broader population. Your situation may sit within the narrower group where the evidence is more supportive.
If steroids were offered as a general next step after failed transfers, without that specific clinical picture behind them, the assessment is useful information to bring into the conversation with your consultant about what the reasoning is and whether it applies to you.
The regulator’s work is designed to inform that conversation, not replace it.
Can Implantation Failure Be Prevented?
A failed transfer does not reveal one cause that can simply be removed before the next attempt.
Some factors are already fixed. The embryo has been created, the egg and sperm have contributed to its development and that transfer has already taken place.
Other factors remain open to review or change. These may include the uterine cavity, lining preparation, progesterone exposure, transfer timing and which embryo is selected next.
Each test examines a specific part of the implantation picture. None can assess the full maternal environment in which implantation must continue.
Implantation has 5 distinct phases and each has to complete successfully for pregnancy to continue.
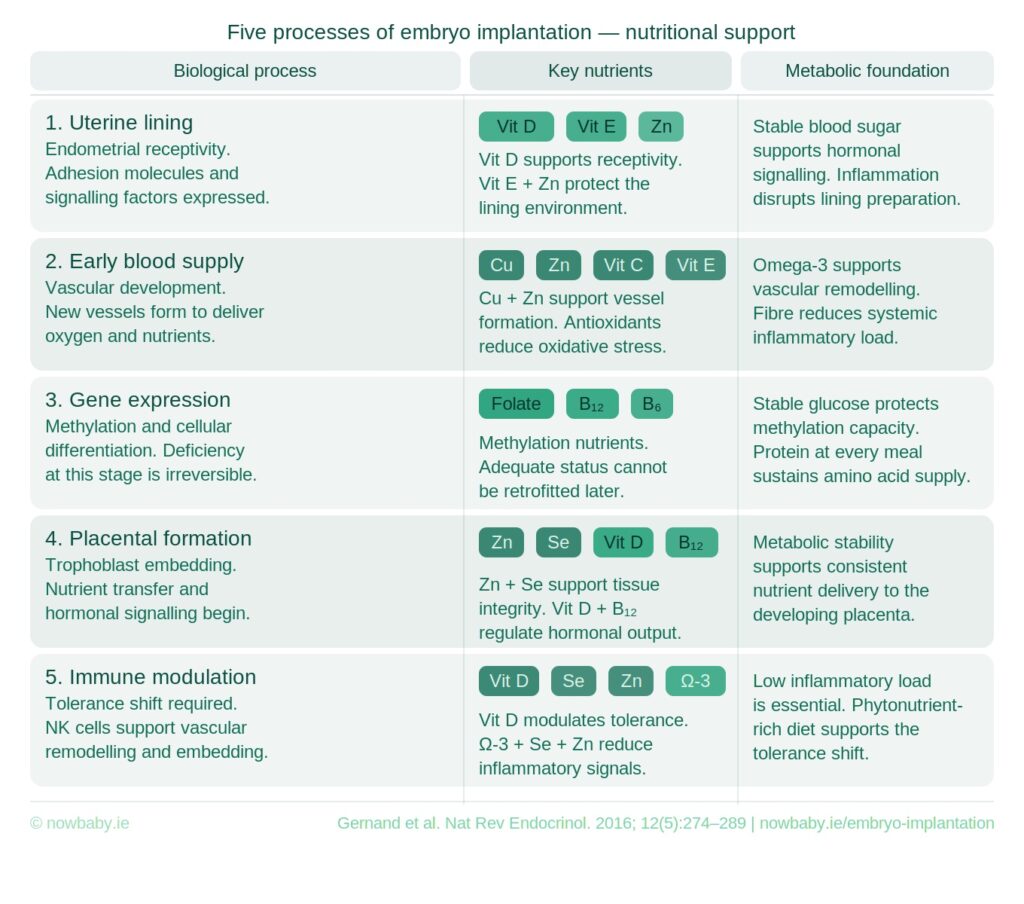
During the days between embryo transfer and the beta hCG result, biological activity increases rapidly. The embryo continues dividing while its cells begin taking on different roles in the developing embryo and the structures that will support the pregnancy.
Each new cell must produce energy, copy DNA, build proteins and cell membranes and respond to signals from surrounding cells. As cell division and differentiation accelerate, the demand for energy and nutrients rises with them.
Amino acids are used to build proteins and new tissue. Fatty acids contribute to cell membranes and cellular signalling. Vitamins and minerals are involved in DNA synthesis, methylation, antioxidant defence, immune adaptation and early vascular development.
Metabolic stability influences how energy is supplied and used during this period. The nutritional demand created by this level of cellular activity extends beyond a supplement routine.
The days between transfer and beta are a period of increased nutritional demand while implantation and early development are underway.
Your next transfer
The two weeks after your last transfer were some of the hardest you will have experienced. Watching the days pass. Trying to hold hope and manage fear at the same time. And then the result that brought you here.
What most women carry out of that experience is the question of whether they did enough. Whether there was something more they could have done.
For your next transfer, the nutritional demands of those fourteen days can be planned for before the two-week wait begins.
Your clinic is planning your transfer with precision, you can apply the same focus to the implantation phase .The role of specific nutrients is critical to your success, and you have an opportunity to support this intentionally.
The Now Baby FET Implantation Meal Plan was built around every one of them.