
")
Anti-Müllerian hormone (AMH) is now one of the most commonly used blood tests in fertility care.
It is frequently presented as a way to assess ovarian reserve, predict future fertility, estimate time pressure, and guide decisions about egg freezing or IVF.
Yet despite how routinely it is measured and discussed, AMH was never validated as a test of natural fertility, time to pregnancy, or reproductive potential.
This is not a matter of interpretation. The American College of Obstetricians and Gynecologists (ACOG) advises that AMH testing should not be used to counsel women without infertility about their future fertility or likelihood of pregnancy.
AMH can provide useful information in specific clinical settings — particularly IVF planning — but when it is used outside that context, it is often misunderstood and over-weighted.
Understanding what AMH can explain, and what it cannot, is essential before major fertility decisions are made.
What AMH Actually Measures
AMH is produced by granulosa cells of small, growing follicles in the ovary.
It reflects current follicular recruitment and ovarian activity in the present moment.
It does not measure egg quality, egg health, genetic integrity, mitochondrial function, or the likelihood of conception.
Put simply:
AMH tells us how the ovary is behaving right now — not how many eggs remain, and not how likely pregnancy is to occur.
Ovarian reserve itself is a theoretical concept. It cannot be directly measured — only inferred.
AMH is one such inference. It is not destiny.
AMH Does Not Predict Time to Pregnancy
One of the most persistent myths surrounding AMH is that a lower value means it will take longer to conceive.
This is not supported by the evidence.
Large population studies and professional guidelines show that, in women without a diagnosis of infertility, AMH levels do not predict how long it will take to become pregnant.
The American College of Obstetricians and Gynecologists’ (ACOG) states clearly that a single serum AMH measurement does not appear to be useful in predicting time to pregnancy.
In practical terms, women with low AMH and women with average AMH conceive at similar rates over time, provided they are ovulating and there are no other limiting factors.
Ovulation requires one egg, not many.
AMH reflects how many follicles are actively maturing, not whether the egg released in a given cycle is capable of resulting in pregnancy.
Why AMH Became So Influential
AMH is useful — but in a very specific context.
It predicts ovarian response to stimulation in IVF.
Higher AMH generally correlates with more follicles responding to medication and more eggs retrieved per cycle. Lower AMH generally correlates with fewer follicles recruited, fewer eggs retrieved, and fewer embryos available within a single IVF cycle.
IVF is a process with multiple stages of attrition. Not every retrieved egg will be mature. Not every mature egg will fertilise. Not every fertilised egg will develop into a transferable embryo. Each step narrows the funnel.
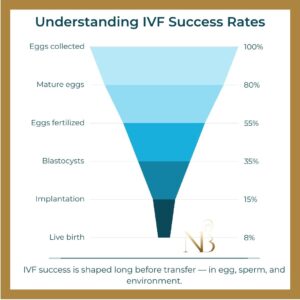
Illustrative IVF attrition funnel. Percentages show the approximate proportion remaining from the original eggs collected; individual outcomes vary.
Because AMH is linked to the number of eggs that enter this funnel, it became a convenient proxy for expected IVF efficiency.
What AMH does not predict is whether pregnancy is possible — only how many opportunities IVF may generate within a given cycle.
This distinction is often lost when AMH is discussed outside IVF planning. A lower AMH can mean fewer attempts per cycle in IVF, but it does not describe egg quality, embryo competence, or the likelihood of conception overall.
IVF Response Is Not Fertility Capacity
IVF is a technology designed to stimulate the ovaries to mature many eggs at once.
When AMH is low, that strategy becomes less efficient.
Fewer eggs retrieved can mean fewer embryos and fewer chances within that particular IVF cycle.
This reflects a technical limitation of IVF — not a verdict on whether pregnancy is possible.
In natural conception, the body is not attempting to mature 10–15 eggs simultaneously. It is trying to ovulate one competent egg in a supportive environment.
IVF outcomes are strongly influenced by the number of eggs available for retrieval. Natural conception requires one egg to ovulate at the right time, with the physiology needed for fertilisation and implantation.
These are fundamentally different biological problems.
Why IVF Is Not Automatically the Best First Step for Low AMH
For women with low AMH and no other identified barriers to conception, IVF may involve high financial cost, significant physical burden, lower egg yield, and emotional pressure around being labelled a “poor responder”.
At the same time, IVF does not address many of the factors that influence natural conception, including egg quality, endocrine environment, ovulation regularity, sperm contribution, and metabolic or inflammatory factors.
In these situations, IVF can become a numbers-driven intervention applied to a problem that is not primarily about numbers.
A low AMH result should not automatically lead to the question:
“How soon should I start IVF?”
It should prompt broader questions about fertility as a whole, including whether ovulation is occurring regularly, whether egg and sperm quality are being supported, and whether intervention is necessary now or whether time is still available.
IVF is one possible tool, but it should not automatically be the first step — nor framed as the only remaining option.
Why AMH Is So Often Misused
AMH produces a number. Numbers feel definitive. Definitive numbers create urgency.
When AMH is treated as a fertility forecast rather than a physiological snapshot, it can distort decision-making and push people toward intervention before it is truly indicated.
This is not a problem with the test itself.
It is a problem with how the test is interpreted and applied outside its validated role.
Why This Matters for Egg Freezing Decisions
AMH is frequently used to justify early egg freezing.
Yet egg freezing success depends far more on age at freezing, number of eggs retrieved, and downstream attrition across thawing, fertilisation, embryo development, and transfer than on AMH itself.
When AMH is treated as destiny rather than context, it can create urgency where proportional decision-making would be more appropriate.
If you are considering egg freezing, it is important to understand how success rates are framed, and where AMH fits — and does not fit — into that picture.
A More Proportional Way Forward
AMH is not meaningless — but it is not predictive in the way many people are led to believe.
It is a marker of ovarian response to IVF, not a forecast of fertility.
Useful in IVF planning. Limited in predicting natural conception. Insufficient on its own to justify urgency, egg freezing, or IVF.
When AMH is treated as destiny rather than context, it distorts decision-making.
Fertility decisions deserve proportional information: an understanding of what a test can explain, what it cannot, and where it fits within the wider reproductive picture.
Single numbers should not be asked to carry life-changing weight.
Clarity does not remove uncertainty — but it restores choice.
Finding a way forward with targeted nutrition
Follicles are metabolically active structures providing the energy and nutrients your egg needs while it is maturing, ready for fertilization. Even after ovulation, their role continues as they produce the progesterone needed to sustain the pregnancy. An egg maturing towards ovulation develops over several months, including approximately 90 days in which your meals, nutrient intake, sleep and metabolic health influence its development. Your partner’s sperm follows a similar cycle.
Targeted nutrition can support that process for both of you.
The Now Baby 90-Day Low AMH Nutrition Protocol is professionally designed around that window — nutrient-dense, blood sugar-balancing, and deliberately constructed to support the cellular conditions that egg and sperm quality depend on.





