

The transfer is booked. Your embryo is ready. And somewhere in the paperwork, Embryo Glue has appeared — an addition to the transfer medium that your clinic says may help the embryo attach.
It is a small thing to say yes to. A substance added to the fluid surrounding your embryo at the moment of transfer, designed to make that first contact with the lining more likely to hold. The cost is relatively modest compared to everything else you have spent to get here. And when you have done everything else, saying yes to one more thing — however uncertain the evidence — can feel like the only rational response.
The Human Fertilisation and Embryology Authority, the UK’s independent fertility regulator, formally assesses the add-ons offered alongside standard IVF. Their evidence reviews are used internationally by clinicians and patients trying to understand what the research actually shows.
EmbryoGlue is on that list.
What Embryo Glue is
Embryo Glue is a hyaluronate-enriched embryo transfer medium. Hyaluronate — more commonly known as hyaluronic acid — is not a synthetic additive. It is a molecule that occurs naturally in the body, including in the fluid that surrounds the embryo during its early development and in the uterine lining in the days around implantation.
Levels of hyaluronic acid in the uterus rise naturally at the time of implantation. The body uses it as part of the environment that supports embryo attachment — it is detected by receptors on both the embryo and the endometrium, and plays a role in helping the embryo locate and adhere to the lining.
The Embryo Glue medium concentrates this molecule at a higher level than standard transfer media contain. The embryo is placed in the medium for at least ten minutes before transfer. When it is loaded into the catheter, some of the medium is transferred into the uterus along with it.
The hypothesis is that by raising the hyaluronic acid concentration at the point of transfer, the embryo arrives in a biochemical environment closer to the natural conditions at implantation — and the initial adhesion signals between embryo and endometrium are amplified at the critical moment.
Is it safe?
Hyaluronic acid is naturally present in the body and the reproductive system. No adverse effects from its use in transfer media have been documented in the clinical literature. Some studies have noted a slight reduction in miscarriage rates alongside the improvement in implantation rates, though this has not reached statistical significance across the full data set. The procedure itself is identical to a standard transfer — Embryo Glue adds nothing to what happens physically.
Safety is not the reason the evidence is conflicting. Efficacy is.
What the regulator assessment shows
The HFEA reviews each add-on against the evidence for whether it improves the chance of a live birth.
Embryo Glue carries a yellow rating — meaning the evidence is conflicting. Some studies have shown benefit, others have not. The picture is more positive than most add-ons in the HFEA review, but not consistent enough to support routine use across all patients.
The conflict becomes clearer when fresh and frozen cycles are examined separately. In fresh IVF transfer cycles, studies have shown a consistent signal of benefit — live birth rates rising from around 33% to 40% across a large body of trial data. In frozen embryo transfer cycles, the picture is contradictory — some studies show significant improvement, others show no effect at all. The yellow rating reflects that unresolved picture.
The clinical situations where Embryo Glue has shown clearest benefit are specific:
- Fresh IVF transfer cycles, particularly in women aged 35 and over
- Women with a history of recurrent implantation failure or unexplained infertility
- Women with diminished ovarian reserve where each embryo represents a significant investment — the limited cohort situation where every marginal gain matters
- Situations where the lining environment at transfer has been a concern in previous cycles
If you are preparing for a frozen embryo transfer and do not fit those categories, the conversation worth having with your clinic is what the specific rationale is for recommending it in your case.
The regulator’s work is designed to inform that conversation, not replace it.
What attachment alone cannot do
Embryo Glue supports the moment of transfer. The biology that follows depends on the environment the body is carrying into those days.
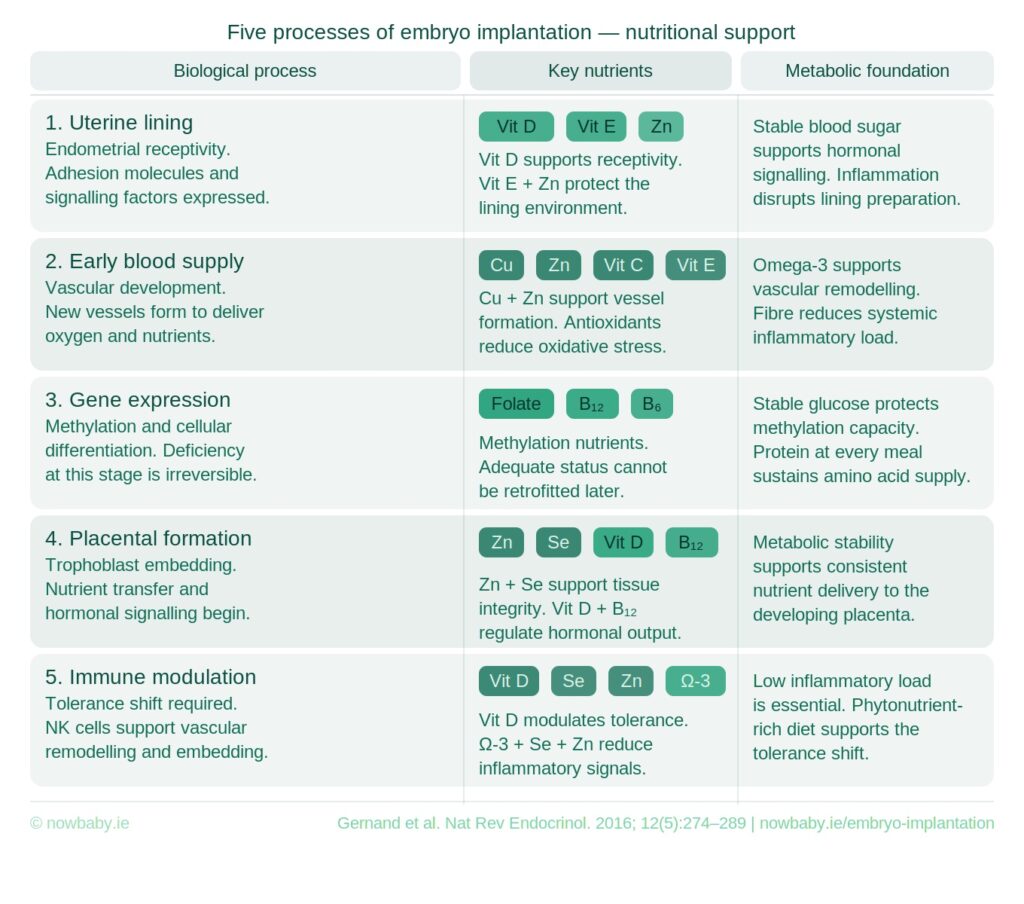 When your embryo attaches, the next step is to embed — establishing the first physical relationship with the maternal blood supply. From there, early blood supply must follow to sustain it. The immune environment of the uterus must modulate to tolerate it. The earliest stages of placental formation must begin.
When your embryo attaches, the next step is to embed — establishing the first physical relationship with the maternal blood supply. From there, early blood supply must follow to sustain it. The immune environment of the uterus must modulate to tolerate it. The earliest stages of placental formation must begin.
That part is yours.
Almost 2 in 3 frozen transfers do not result in a live birth — not because the embryo was wrong, not because the transfer was wrong, but because implantation is a biological process that responds to the environment it meets. That environment is shaped by nutrition, hormonal steadiness, inflammatory load, blood flow and metabolic health. None of those are addressed by what happens in the transfer room.
Embryo implantation has 5 distinct phases and each has its own nutrient requirements, Your embryo needs to embed into the lining, establish an early blood supply, begin placental formation and negotiate immune tolerance — all before a test can confirm anything. Each of those phases responds to what the body has been given to work with.
The Now Baby FET Implantation Meal Plan was designed around every one of those phases — the nutritional structure for the days your biology is doing its most demanding work. Professionally analysed. Beginning the day after transfer.
You didn’t come this far to wing it.





