

Progesterone suppositories are progesterone medication administered via the vagina in some frozen embryo transfer cycles.
Your clinic may prescribe them before embryo transfer, after embryo transfer, or both, depending on your own protocol.
A suppository is designed to soften after insertion. Progesterone is released as the base softens and is absorbed via the vaginal wall. Some of that softened base can then mix with vaginal fluid and appear later as discharge or residue.
That residue can look like medication has leaked out and you may be concerned that your dosage is affected. Seeing residue does not mean the progesterone dose has failed.
Why clinics prescribe progesterone suppositories in FET
In an ovulatory cycle, progesterone rises after ovulation.
That rise matters because progesterone helps move the endometrium into the receptive phase needed for implantation.
A fully medicated FET protocol is different.
Ovulation is usually suppressed, so there is no corpus luteum providing progesterone for the lining. The cycle does not create its own post-ovulation progesterone rise.
Progesterone medication replaces that missing source.
This is why progesterone may be started before embryo transfer. The lining needs progesterone acting on it before your embryo is placed into the uterus. Progesterone is usually continued after transfer because the endometrium still needs progesterone support while the embryo and lining move into the implantation window.
Progesterone suppositories are one option for providing that medication. Some cycles use vaginal progesterone alone. Others use more than one progesterone form.
The reason is the same: the lining needs progesterone before transfer and continued progesterone support after the embryo is placed into your uterus.
Discharge and leaking after progesterone suppositories
Progesterone suppositories soften after insertion.
As the base softens, progesterone is released and absorbed through the vaginal wall. Some of the softened base can then mix with vaginal fluid and appear later as discharge or residue.
That residue can look like leaking. It may look white, creamy, chalky, oily or watery. It may show on underwear, a liner or tissue, appear when you wipe, or become more noticeable after standing, walking, changing position or using the toilet.
Movement can make residue more noticeable. Softened base that has been sitting in the vagina may move down and appear on a liner, tissue or underwear.
The amount can vary from dose to dose. One dose may leave very little residue. Another may leave a heavier mark.
More visible residue does not reliably mean that less progesterone has been absorbed. It usually means more softened base and vaginal fluid have moved out after the suppository has softened.
Does leaking mean the dose has not absorbed?
Leaking after a progesterone suppository does not usually mean the dose has not absorbed.
Residue that appears later, after the suppository has softened, is different from a suppository that comes back out whole or nearly whole soon after insertion.
A softened suppository has already released progesterone from its base. The residue that appears later is usually the remaining softened base mixed with vaginal fluid.
A suppository that comes back out whole or nearly whole soon after insertion is different. In that situation, the question is whether it stayed in place long enough to soften and release progesterone.
Irritation, soreness and vaginal discomfort
Vaginal progesterone can cause local irritation because the medication is being used directly inside the vagina.
The tissue is exposed to the suppository, the softened base, residue, moisture and repeated insertion. Over several days, that can leave the vaginal opening and surrounding vulval skin feeling more sensitive.
Irritation may feel like stinging, burning, itching, rawness, tenderness, swelling, or a bruised feeling around the vaginal opening. The discomfort may be inside the vagina, on the vulval skin, or both.
Residue can add to the problem when it sits against the skin. Moisture on a liner can rub. Extra wiping can also make the area feel more sore, especially when the skin is already irritated.
Liners can help contain discharge, but they can become part of the irritation if they stay damp or rub against sensitive skin. Changing them when needed and patting rather than rubbing can reduce friction.
The aim is not to scrub away every trace of residue. It is to keep the area as comfortable as possible while you continue the medication as prescribed. Using the insertion method described in your product instructions can also make repeated use easier to manage.
Intercourse while using progesterone suppositories
Intercourse can feel different when progesterone is being used vaginally in a frozen embryo transfer cycle.
The suppository base softens after insertion and can leave residue or discharge. That residue may be present inside the vagina or around the vaginal opening. Repeated use can also make the vaginal tissue and surrounding vulval skin more sensitive.
That can change how sex feels.
It may feel messier than usual because of discharge or softened base. It may feel drier, more tender, stingy or irritating because the tissue has already been exposed to medication, residue, moisture, wiping, liners or repeated insertion.
Friction can make soreness more noticeable. If the vulval skin or vaginal opening is already irritated, intercourse may feel uncomfortable in a way that has nothing to do with desire or emotional connection. It is a physical effect of using medication in a sensitive area every day.
That physical change can matter emotionally too. In a FET cycle, intimacy is happening alongside medication timings, transfer instructions and the pressure of not wanting to get anything wrong. Residue, discharge or soreness can make sex feel less straightforward than it normally would.
If your clinic has given you specific instructions about sex before or after embryo transfer, follow those instructions for your own cycle.
Symptoms after transfer are hard to read
After embryo transfer, you will want to know whether implantation has happened as early as possible.
That is why every sensation can feel loaded with meaning. Cramping, bloating, breast tenderness, fatigue, headaches, nausea, discharge, spotting or mood changes can all feel significant because they arrive at the point when you are looking for signs from your body.
Progesterone is one reason those signs are difficult to read.
Vaginal progesterone can cause breast tenderness, bloating, headaches, tiredness, mood changes, nausea, discharge and local irritation. Those symptoms can overlap with the effects of oestrogen medication, the transfer procedure, normal pelvic sensitivity and early pregnancy changes.
This is why symptoms after transfer are not a reliable way to read implantation.
The same symptom can have more than one explanation. Cramping can feel hopeful one hour and worrying the next. Discharge can come from vaginal progesterone rather than implantation. Breast tenderness and fatigue can come from medication before a pregnancy test can give any clear answer.
The absence of symptoms can be just as unsettling. Implantation does not create one clear symptom pattern that every woman can feel or identify.
After transfer, symptoms can tell you what you are experiencing. They cannot confirm whether implantation has happened.
Your clinic’s pregnancy test is the point that gives clearer information.
When to contact your clinic
Progesterone suppositories can cause discharge, residue and local irritation. They can come from how vaginal progesterone is used: the suppository softens, leaves residue behind, and exposes sensitive tissue to repeated contact.
Some changes need clinic guidance because they are not ordinary suppository residue.
Bleeding is one of them. Light spotting can happen after embryo transfer, but bleeding still needs to be interpreted in the context of your transfer timing, medication plan and history.
Contact your clinic promptly if bleeding becomes heavier, bright red, painful, or comes with dizziness.
You should also contact your clinic if you have strong pelvic pain, fever, painful urination, discharge with a concerning smell, a rash, swelling, breathing symptoms, chest pain, visual changes, or a severe headache.
Medication issues need a different response from ordinary leakage. A missed dose, a dose used at the wrong time, a suppository that comes straight back out, or running short of progesterone are not the same as residue appearing after a suppository has softened.
Those situations cannot be judged from residue on a liner. They need your clinic’s guidance because they involve the medication plan itself, not ordinary leakage after a suppository has softened.
The limitations of progesterone suppositories
Progesterone suppositories do one specific medication job in a frozen embryo transfer cycle. They provide progesterone to help prepare and maintain the uterine lining for embryo implantation.
That is important, but it is not the full implantation process.
Implantation is wider than progesterone alone. It has 5 distinct phases and each has its own nutrient requirements.
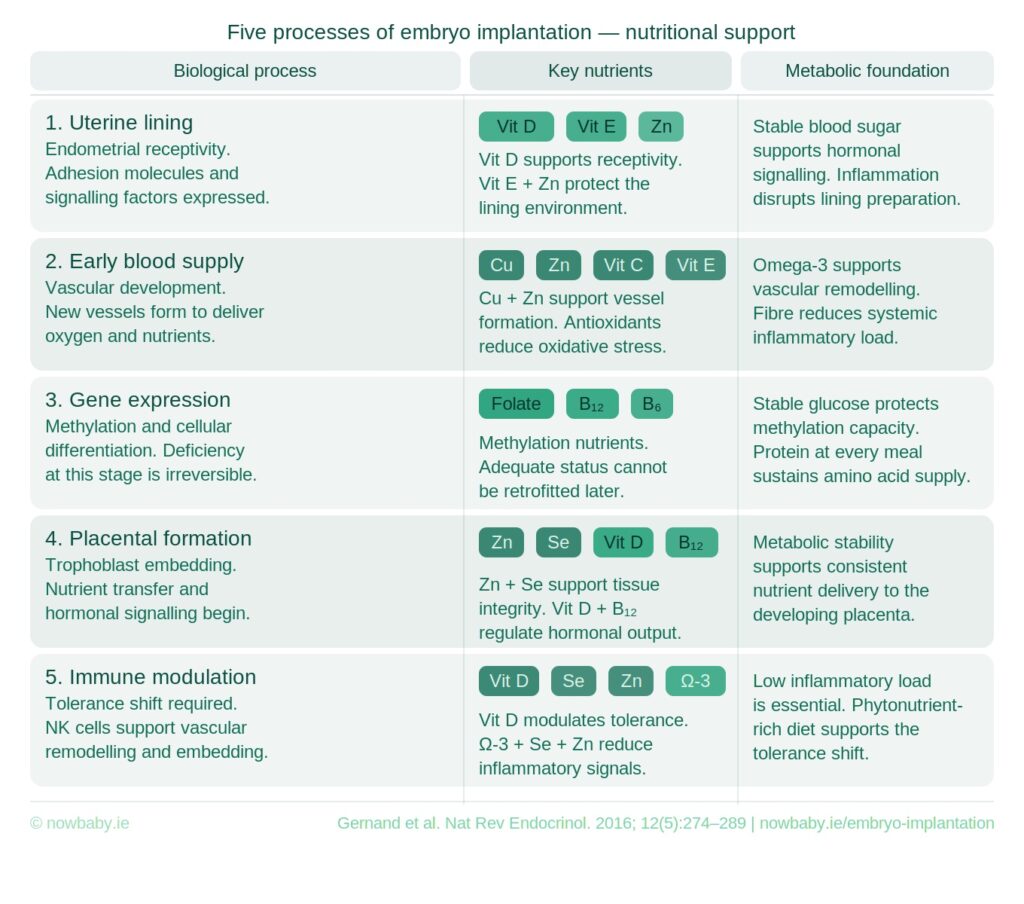
Progesterone supports the lining environment for implantation. It does not cover the full nutritional and physiological demands of the implantation process.
The Now Baby FET Implantation Support Meal Plan is designed to support the next phase: targeted nutrition for the 5 stage implantation process after frozen embryo transfer.

Get the FET Implantation Support Meal Plan





