

PIO Shots vs Progesterone Suppositories for FET: Is One Better?
PIO shots and progesterone suppositories are two progesterone routes used in frozen embryo transfer cycles.
PIO stands for progesterone in oil. It is usually given as an intramuscular injection.
Progesterone suppositories are progesterone medication administered via the vagina in frozen embryo transfer cycles.
Neither route is automatically better in every FET cycle. They deliver progesterone differently, and each route belongs inside a wider protocol that includes dose, timing, embryo stage, cycle type and clinic monitoring.
The comparison starts with the job progesterone is doing.
In FET, progesterone is used to move the endometrial lining from oestrogen-led growth into the receptive phase needed before your embryo is transferred.
A lining can look thick enough on scan and still need the correct progesterone exposure before transfer. Thickness is structure. Progesterone changes function.
It affects timing, secretions, gene activity, tissue response and the opening of the implantation window.
That is why the route cannot be judged on its own.
PIO and suppositories are not two simple strength levels. They are two delivery routes for the hormone your lining needs to be exposed to at the right time.
Why progesterone support matters in FET
In an ovulatory cycle, progesterone rises after ovulation.
That rise comes from the corpus luteum, the temporary hormone-producing structure left behind after the follicle releases the egg.
Before ovulation, oestrogen helps the endometrial lining grow. After ovulation, progesterone changes the lining from a growth phase into a secretory, receptive phase.
The lining is not simply becoming thicker.
It is changing what it can do.
Progesterone changes the glands within the endometrium. It affects the molecules released into the uterine cavity. It helps regulate the timing of the implantation window, when the lining is most able to respond to an embryo.
That timing is central to FET.
In a fully medicated FET, ovulation is usually suppressed or bypassed. The body’s usual post-ovulation progesterone source is not providing the main support, so the clinic has to prescribe and time progesterone deliberately.
In a natural or modified natural FET, ovulation may create a corpus luteum. Your clinic may still prescribe progesterone support to strengthen or standardise the luteal phase around transfer.
The protocol is designed to line up two things:
your embryo’s stage of development
and your lining’s progesterone exposure.
A blastocyst is not transferred into a lining that has only just started receiving progesterone. The clinic counts progesterone exposure because the lining changes over time.
Too little exposure can leave the lining behind the embryo.
Too much exposure can move the lining ahead.
The timing matters.
This is why progesterone instructions are not background medication. They are part of the transfer protocol itself.
How PIO shots deliver progesterone
PIO works through systemic progesterone exposure.
The progesterone is carried in oil, so it does not move into the bloodstream all at once. After the injection, the oil base holds progesterone in the muscle and releases it gradually into the circulation.
From there, progesterone reaches the uterus through the blood supply.
The endometrial lining has progesterone receptors. Once the lining is exposed to progesterone, the cells in that tissue begin to behave differently. The glands become more secretory. The lining becomes more closely timed to the embryo stage. The implantation window begins to open according to the number of progesterone exposure days before transfer.
In a fully medicated FET, this matters because ovulation is usually suppressed or bypassed.
There may be no corpus luteum providing the body’s usual post-ovulation progesterone rise. The clinic is creating that hormonal phase with medication.
PIO gives the clinic a systemic route for that support.
If serum progesterone monitoring is used, the blood result gives one measure of circulating progesterone. It does not show every detail of how the lining is responding, but it can help the clinic assess progesterone exposure within its own protocol.
The injection route can be physically difficult.
The oil base can irritate muscle tissue and leave soreness, bruising, tenderness, swelling or small lumps. These effects can make the cycle harder to tolerate, especially when injections are daily.
That physical load is real. It affects comfort and tolerance during the cycle.
Within the FET protocol, PIO’s job is progesterone exposure over time. It provides a bloodstream route for the hormone that helps the endometrium move into the progesterone-led phase planned before transfer.
How progesterone suppositories deliver progesterone
Vaginal progesterone does not rely on the same bloodstream route as PIO.
After insertion, progesterone is absorbed through the vaginal tissue. From there, it can reach the reproductive tract through local blood vessels and tissue pathways close to the uterus.
That closeness matters.
With PIO, progesterone enters the wider circulation first and then reaches the uterus through the blood supply.
With vaginal progesterone, the route is more local. The uterus can be exposed to progesterone even when the level measured in the bloodstream does not look the same as it might after an intramuscular injection.
This is why the two routes should not be compared as if they are simply stronger and weaker versions of the same delivery method.
They move progesterone through the body differently.
For the endometrial lining, the key issue is still progesterone exposure over time.
The lining has progesterone receptors. Once those receptors are exposed to progesterone over the planned number of days before transfer, the tissue begins to move into the progesterone-led phase needed for a frozen embryo transfer.
The glands in the lining become more secretory. The tissue becomes more closely timed to the embryo stage. The implantation window is shaped by that timed exposure before transfer.
Vaginal progesterone gives the clinic a local route for creating that exposure.
With suppositories, progesterone reaches the reproductive tract through vaginal absorption rather than first moving from muscle into the wider bloodstream.
That local route is why blood progesterone levels may not mirror PIO, even when the uterus is being exposed to progesterone.
Why clinics choose different protocols
Progesterone protocols vary because FET cycles are not all built the same way.
In a fully medicated FET, ovulation is usually suppressed or bypassed. The clinic has to create the progesterone phase with medication because there may be no corpus luteum providing the body’s usual post-ovulation rise.
In a natural or modified natural FET, ovulation may still happen. The corpus luteum may contribute progesterone, and medication may be added to support or standardise the luteal phase around transfer.
Those are different hormonal starting points.
Embryo stage also matters. A blastocyst transfer is timed around a defined number of progesterone exposure days before transfer. The lining and embryo need to be matched in time, not just brought together in the uterus.
Monitoring policy adds another layer.
Some clinics check serum progesterone before transfer. Some adjust support if blood levels fall below their threshold. Others use a standard protocol based on cycle type, medication route and their own outcome data.
Route choice sits inside that wider system.
PIO gives progesterone through a systemic bloodstream route. Vaginal progesterone gives a more local route close to the reproductive tract. A combined protocol may be used when a clinic wants both forms of exposure or when previous monitoring has raised concern.
That does not make one route the universal answer.
It means the route only makes sense when the full protocol is considered: whether ovulation occurred, whether a corpus luteum is present, when progesterone started, how many exposure days the lining has before transfer, what embryo stage is being transferred and whether the clinic is monitoring progesterone levels.
This is why route choice cannot be separated from cycle design.
A medicated FET without a corpus luteum, a natural or modified natural FET with one, a monitored cycle with serum progesterone thresholds, and a blastocyst transfer timed to defined progesterone exposure days are not the same clinical situation.
The protocol is built around those differences.
What you can support during the implantation window
By transfer day, progesterone has already been doing a specific job.
It has helped prepare the endometrial lining. The lining is not being prepared for thickness alone. It is being timed for contact with your embryo.
Embryo transfer then places your embryo into the uterus.
The 5 phases of implantation come next.
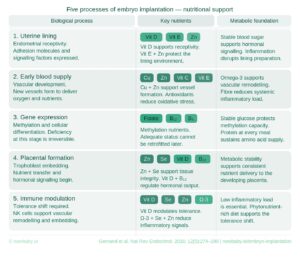
Secure implantation into the lining, early blood supply, gene expression and differentiation, placental formation and immune adaptation.
Secure implantation into the lining is first contact becoming more than contact.
The blastocyst has to settle against the endometrial surface. Cells on the outer layer of the embryo attach to the lining and begin moving into the upper layer of maternal tissue. The lining has to remodel around that contact, so your embryo is not simply resting in the uterus. It is beginning to embed.
Early blood supply has to start developing around that interaction.
Progesterone helps prepare the lining for this window.
The implantation process itself uses nutrients to support cell division, tissue remodelling, blood-supply signals, gene activity, early placental tissue development and immune activity adaptation.
That is the part nutrition can support.
Nutrition provides the building blocks for this critical phase.
The progesterone protocol prepares and supports the lining.
The days after transfer ask more of the body than lining preparation alone.
Nutrients for life
Each of the five implantation phases has a specific nutritional demand. The fourteen days after transfer are when those demands are active. This is not a window where general healthy eating or supplements are enough.
The Now Baby FET Implantation Meal Plan is built around exactly that window. Every meal across the fourteen days has been designed around the nutritional demands of the implantation window — every process, every nutrient, every day — professionally analysed and structured so that the one variable that remains within your control is no longer left to chance.
You have optimised everything your clinic controls. This is the part only you can do.
Get the FET Implantation Support Meal Plan.





